SARS-CoV and MERS-CoV: Understanding Two Major Coronaviruses
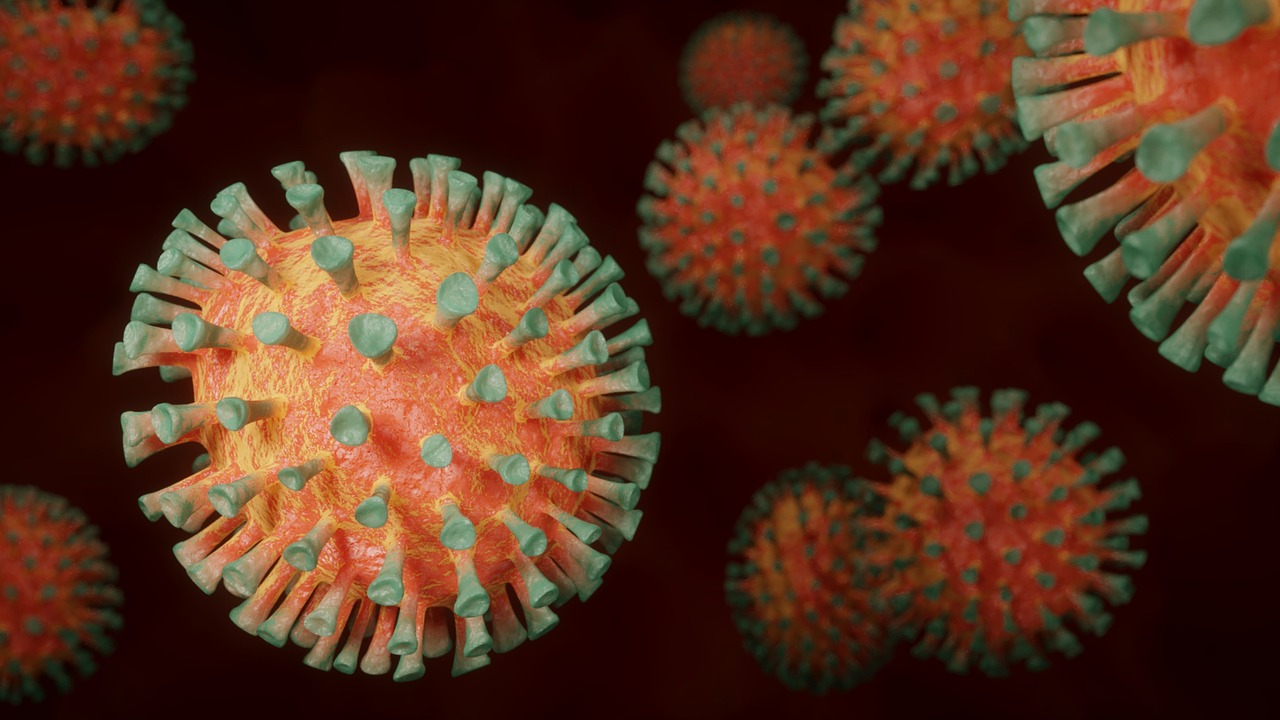
Coronaviruses are enveloped, single-stranded, positive-polarity RNA viruses with a helical nucleocapsid structure. They lack virion polymerase and feature club-shaped spikes that form a "corona" visible under an electron microscope. The coronavirus genome sequence that caused the 2002 SARS (Severe Acute Respiratory Syndrome) outbreak differs from existing human strains, making it difficult to analyze and devise a defensive strategy.
Coronavirus is a major cause of the common cold, second only to rhinovirus. In 2002, SARS-CoV emerged, followed by the appearance of MERS (Middle East Respiratory Syndrome) in 2012. These diseases are caused by SARS-CoV and MERS-CoV, respectively. Both syndromes are types of viral pneumonia. A new strain of coronavirus emerged in December 2019 in Wuhan, China, leading to the COVID-19 pandemic. Millions of lives were lost, and while vaccines helped reduce infection rates, the virus's ability to mutate and produce new strains continues to pose challenges.
Transmission and Reservoirs
Coronaviruses are primarily transmitted through respiratory aerosols, enabling human-to-human transmission. People infected with SARS were identified as "super-spreaders." Early in the SARS outbreak, many healthcare workers were infected, but following proper respiratory infection control procedures helped mitigate the spread.
Animals, particularly horseshoe bats, are natural reservoirs for SARS-CoV, with civet cats serving as intermediate hosts. MERS-CoV, on the other hand, is closely related to bat coronaviruses, and bats are considered the main reservoir for MERS-CoV.
Mechanism of Action
Once inside the body, the virus adsorbs to cells via surface spikes and penetrates the cytoplasm. After uncoating, the positive-strand RNA genome is translated into polypeptides that self-cleave via virus-encoded proteases. RNA polymerase is then formed, allowing genome replication. Additional mRNAs are synthesized and translated into structural proteins, and the virus assembles in the cytoplasm, acquiring its envelope from the endoplasmic reticulum.
After release from cells, the virus primarily infects the mucosal cells of the respiratory tract. SARS-CoV attaches to ACE-2 receptors on respiratory tract epithelium, leading to fluid imbalance and edema in alveolar spaces, resulting in hypoxia, a hallmark of SARS-induced pneumonia. MERS-CoV, however, binds to CD-26 receptors on respiratory mucosa.
Symptoms and Diagnosis
Symptoms of SARS and MERS include severe atypical pneumonia, high fever (38°C or higher), non-productive cough, dyspnea, and hypoxia. Other common symptoms include chills, rigors, malaise, and headaches. Sore throat and rhinorrhea are uncommon. The incubation period for both SARS and MERS ranges from 2 to 10 days, with a mean of 5 days. The symptoms of both infections are quite similar.
Diagnosis typically involves a chest X-ray, which reveals interstitial ground-glass infiltrates that do not cavitate. Leukopenia and thrombocytopenia are also commonly observed. If SARS or MERS is suspected, PCR-based tests of blood and respiratory specimens are conducted to confirm the diagnosis.
Treatment and Challenges
There is no specific treatment for SARS and MERS, nor is there an effective vaccine yet. Vaccines are still in development, but results have been mixed. Symptomatic treatment is the mainstay of care. A combination of ribavirin and steroids has been used in life-threatening SARS cases, but its efficacy remains uncertain.
Similar Post You May Like
-
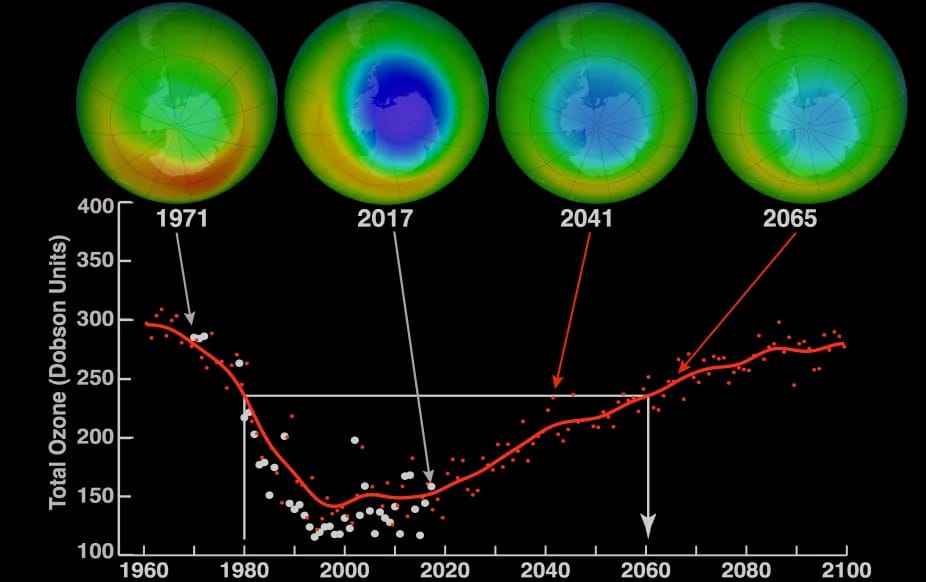
CFCs, HFCs and their long, troubled history
At its peak, the ozone hole covered an area 7 times larger than the size of Europe, around 29.9 million km2, and was rapidly expanding
-

The Origin of Universe: Deciding point where it all began!
Let us unravel and surf through the ideas throughout ages to understand what the universe and its origin itself was to its inhabitants across history.
-

The Artemis Program
Inspired by the Greek goddess of the Moon, twin sister to Apollo, the artimis program was named on 14 May 2019 by Jim Bridenstine.
Recent Post
-
Second Brain in Your Belly? Inside the Fascinating Gut-Brain Connection
Ever wondered why you feel butterflies in your stomach? That gut-wrenching feeling in the pit of your stomach might not be as insignificant as it seems.
-

The AI Arms Race: Boon or Bane for National Defense?
Artificial intelligence (AI) is rapidly transforming industries, and the defence sector is no exception.
-
Unveiling the Oldest Black Hole: A Cosmic Odyssey with the James Webb Space Telescope
In a groundbreaking revelation, astronomers using the James Webb Space Telescope (JWST) have uncovered the existence of the oldest black hole ever discovered
-

Hubble's Iconic Journey into the Depths of the Universe
arguably the greatest technological breakthrough of its time, now have over three decades of service.
-

The Metaverse: Exploring Its Concept, Potential, and Social Implications
The metaverse encompasses a vast and interconnected digital universe where users can interact, create, explore, and collaborate
-
The Man, the Myth, and the Mathematical Legacy
Pythagoras, the enigmatic figure whose name is forever intertwined with the famous theorem, emerges from the mists of ancient Greece as a polymath of profound influence.